
Chapter 3: How people manage anxiety or depression
This is chapter 3 of the Wellcome Global Monitor 2020: Mental Health
Global statistics on the availability of mental health services tend to focus on facilities and personnel specialising in clinical methods. However, people the world over use a much broader range of approaches to manage or address their anxiety or depression (defined as being ‘so anxious or depressed that you could not continue your regular daily activities as you normally would for two weeks or longer’). This chapter takes a closer look at what people worldwide do to help themselves feel better by focusing on the following question:
- When you were feeling so anxious or depressed, did you ever do any of the following to make yourself feel better?
a. Talk to friends or family
b. Improve healthy lifestyle behaviours, such as exercise, sleep and diet
c. Spend time in nature/the outdoors
d. Make a major change in your personal relationships
e. Make a major change in your work situation
f. Take medication as prescribed by a healthcare professional
g. Talk to a mental health professional
h. Engage in religious or spiritual activities, or talk to a religious leader
One of the eight approaches described in the survey was talking to friends and family, and most people said they did this to help deal with their anxiety or depression.
Worldwide, 78% of people who said they have experienced anxiety or depression also said that they talked to family and friends to make them feel better, as shown in Chart 3.1. Improving healthy lifestyle behaviours and spending time outdoors were also chosen by more than 70% of people around the world.
Chart 3.1: Approaches taken to alleviate anxiety or depression, global results
Percentage of people who answered ‘yes’.
When you were feeling so anxious or depressed, did you ever do any of the following to make yourself feel better?
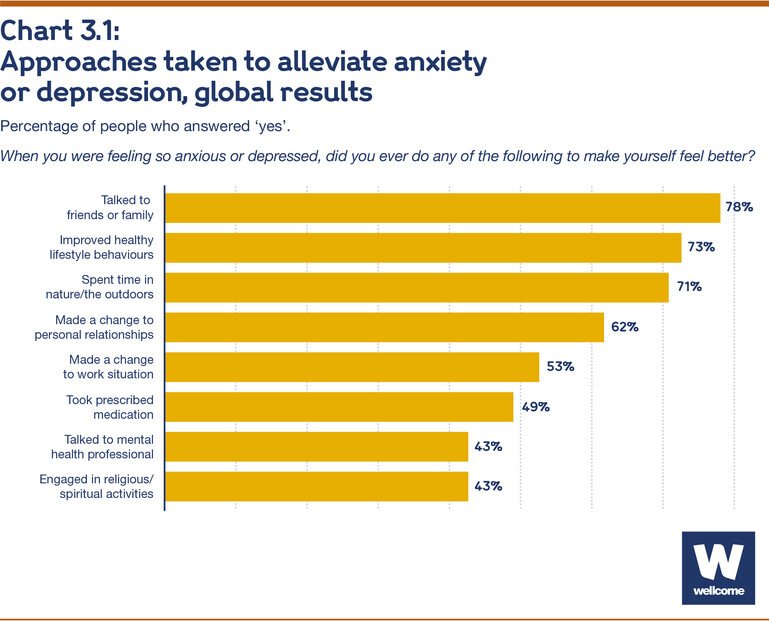
As shown in Figure 3.1, the top two global-level responses – talking to friends or family and improving healthy lifestyle behaviours – were also among the top three responses in every region. Notably, Sub-Saharan Africa and Latin America were the only regions where spending time outdoors was not among the top three responses. In Sub-Saharan Africa, it was replaced by engaging in spiritual or religious activities; in Latin America, people were more likely to say they made a change to their personal relationships.
Figure 3.1: Map showing the most common approaches taken to alleviate anxiety or depression, by region*
Interact with the data in more detail via the chart below
As shown in Figure 3.1 and Table 3.1, at the global level, talking to a mental health professional, taking medication and engaging in religious or spiritual activities were the least-cited methods for feeling better. People in low-income countries and areas were among those most likely to choose religious or spiritual activities, and those in high-income countries were among the most likely to choose taking medication and talking to a mental health professional.
*See Appendix A for complete results by region — Table A.2.
Table 3.1: Approaches taken to alleviate anxiety or depression, by country income group
Percentage of people who answered ‘yes’.
When you were feeling so anxious or depressed, did you ever do any of the following to make yourself feel better?
|
Low-/Lower-middle- |
Upper-middle-income countries |
High-income countries |
|
|---|---|---|---|
| Talked to friends or family | 81% | 74% | 79% |
| Improved healthy lifestyle behaviours | 73% | 72% | 73% |
| Spent time in nature/the outdoors | 67% | 72% | 78% |
| Made a change to personal relationships | 62% | 65% | 58% |
| Made a change to work situation | 59% | 49% | 50% |
| Took prescribed medication | 49% | 41% | 64% |
| Talked to a mental health professional | 36% | 38% | 67% |
| Engaged in religious/spiritual activities | 49% | 41% | 34% |
Regional and country-level differences demonstrate how economic and cultural conditions can influence which actions people take to make themselves feel better:
- People who have experienced anxiety or depression in Sub-Saharan Africa were least likely to say they spent time outdoors or in nature to feel better, at 56%. However, this finding could be the result of people generally spending much of their time outdoors – agriculture is the largest economic sector in the region, employing more than half the region’s workers (1).
- People in the US who have experienced anxiety or depression were among the most likely in any high-income country or area to say they engaged in spiritual or religious activities, at 56%. Notably, the US is an outlier among high-income countries because of its high level of religiosity. In 2020, 60% of Americans said religion was important in their daily lives, compared with an average of 37% across the other 39 high-income countries surveyed. A 2018 Pew survey found that Americans were also more likely than adults in other wealthy Western democracies to say they attend weekly religious services and pray daily (2). Two-thirds of Americans who said religion was important in their daily lives (68%) engaged in religious or spiritual activities to alleviate anxiety or depression, compared with 38% of those who said religion was not important in their daily lives.
- The proportion who tried improving healthy lifestyle behaviours was lowest in the Middle East/North Africa, at 55%. Previous research has identified sedentary behaviour as a serious public health issue in this region: a 2020 meta-analysis found that only about half of the adults in the region (51%) got enough physical activity to avoid risk factors for obesity – well below recent global estimates of 72.5% to 77% (3). The hot climate across the Arabian Peninsula and the Arab Gulf region limits outdoor physical activity to the winter months, and indoor fitness facilities are rare, particularly in lower-income countries (4).
Approaches to alleviating anxiety or depression differed by gender and education level in some regions
As with differences in the likelihood of having experienced anxiety or depression, demographic differences in the actions people with anxiety or depression took to feel better were more pronounced in certain regions and countries than at the global level.
Gender
Similar proportions of men and women around the world tried most of the eight approaches listed in the survey to alleviate anxiety or depression*. However, the regional results show notable gender differences:
- In several regions, women were more likely than men to say they had talked to a mental health professional; these include Northern America (78% of women compared with 61% of men), Latin America (52% compared with 37%), Eastern Europe (49% compared with 37%), Russia/Caucasus/Central Asia (29% compared with 18%) and Australia/New Zealand (79% compared with 71%). In some cases, these gaps probably reflect gender norms that discourage help-seeking behaviour among men (5,6). Prior studies have found that though men are at greater risk of suicide globally, they are less likely to seek mental health support (7).
- Women were also more likely than men in several of these same regions – including Australia/New Zealand, Eastern Europe, Latin America and Russia/Caucasus/Central Asia – to say they took prescribed medication when they experienced anxiety or depression. However, the gender gap for this method was much smaller in Northern America (69% of women compared with 65% of men) than for talking to a mental health professional.
- Men in Northern America were more likely than women to say they improved healthy lifestyle behaviours in response to anxiety or depression – 88% compared with 72%, respectively. The reverse was true in East Asia, where 76% of women said they took this approach, compared with 63% of men.
*The only exception is that men were somewhat more likely than women to make a change to their work situation, but this largely reflects higher formal participation in the workforce among men in many countries.
Education
Globally, people with varying education levels who have experienced anxiety or depression were all likely to have tried most approaches to feeling better. There was one important exception: people with a lower education level were less likely to have spoken with a mental health professional, largely reflecting the difference between low-income and middle-income countries (where average education levels are lower) and high-income countries, as seen in Table 3.1.
However, people’s likelihood of taking prescribed medication was relatively consistent by education level, even though this approach was also more common in high-income countries. Worldwide, 52% of those with a primary level of education or lower (0-8 years) said they took prescribed medication to feel better, compared with 47% of those with a secondary education (9-15 years) and 49% of those with a post-secondary education (16+ years). The global percentage for people with no more than a primary education was relatively high largely because in middle-income and low-income countries, people in the groups with the lowest level of education were most likely to say they took prescription medication to feel better.
Most people tried a mix of approaches to alleviate anxiety or depression
The vast majority of people who have experienced anxiety or depression tried a number of different ways to make themselves feel better. Chart 3.2 shows that 85% said they had tried at least three of the eight actions listed in the survey, compared with 3% who said they had not tried any and 4% who had tried just one. Ten per cent reported taking all eight approaches.
Chart 3.2: Number of approaches people took to alleviate anxiety or depression, global results
Percentage of people who answered ‘yes’.
When you were feeling so anxious or depressed, did you ever do any of the following to make yourself feel better?
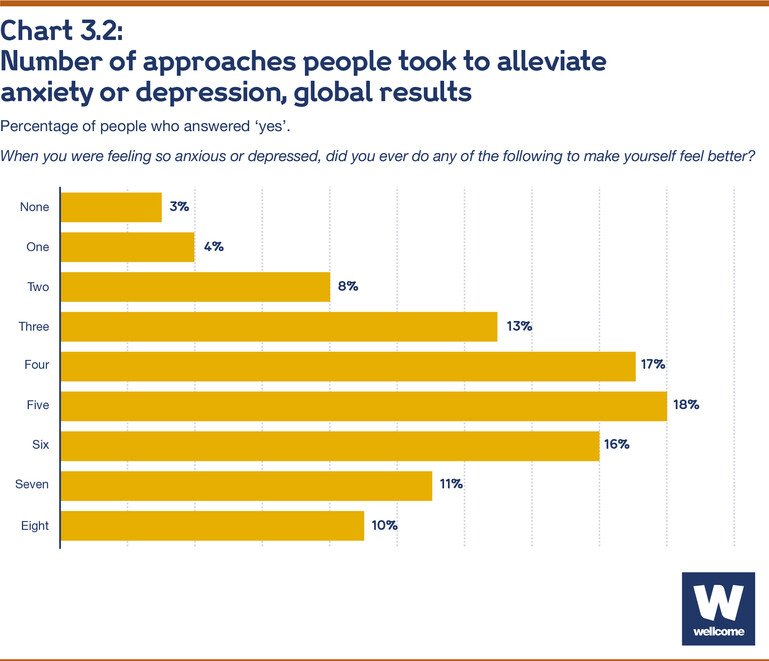
On average, people who have experienced anxiety or depression had tried 4.7 of the eight actions listed in the survey to make themselves feel better. This figure varied little between country income groups, but there were notable differences in some regions of the world. For example, people in Northern America had taken 5.6 of the actions on average, compared with fewer than four among those in East Asia (3.9) and the Middle East/North Africa (3.7).
Several of the countries with the lowest averages are in the Middle East/North Africa region, including Lebanon (2.8), Egypt (3.2), Jordan (3.2), Morocco (3.4), Saudi Arabia (3.5) and Iraq (3.6). As previously noted (see p. 22), people in this region who have experienced anxiety or depression were less likely than those in other regions to try improving healthy lifestyle behaviours. They were also among the least likely in the world to say they talked to a mental health professional (25%), made a change to their work situation (28%)* or took prescribed medication (33%).
*This finding is due in part to the low level of women’s formal participation in the workforce in much of the Middle East and North Africa. Twenty per cent of the women from this region who took part in the survey and who have experienced anxiety or depression said they had made a change to their work situation, compared with 36% of men.
The most common combinations of approaches people took to feel better fell into three ‘clusters’
Some of the actions people who have experienced anxiety or depression took to feel better are commonly associated with one another. A deeper analysis reveals these patterns and identifies the most common sets of approaches people selected.
Findings concerning the specific combinations of commonly used approaches are based on analytical modelling and statistical clustering techniques. See Appendix A for a complete discussion of the cluster analysis and outcomes.
Three primary types of clusters (i.e., large groups of people who used the same specific combination of methods) emerged from the global results – and most regional ones – and are shown in Table 3.2:
Cluster 1, holistic combination
The most widespread cluster comprises a broad combination of approaches, including talking to a mental health professional, improving healthy lifestyle behaviours, spending time outdoors, talking to friends or family, taking prescribed medication and making a change to personal relationships. About 35% of those who have experienced anxiety or depression worldwide used this holistic strategy, but it was most common in high-income regions, including Australia/New Zealand (61%), Northern America (59%) and Western Europe (56%).
Cluster 2, lifestyle changes
The second cluster, used by about 28% of people worldwide who have experienced anxiety or depression, specifically excludes talking to a mental health professional and taking prescribed medication. Rather, it includes a subset of actions from the first cluster that do not require professional input – improving healthy lifestyle behaviours, spending time outdoors and talking to friends or family. This cluster was most commonly used in Southeast Asia (44%), the Russia/Caucasus/Central Asia region (40%) and Latin America (33%).
Cluster 3, primary support from friends or family
The third cluster leans primarily on one approach: talking to friends or family. Most people who used this cluster (60%) have sought social support in this way, while 41% said they have made a change to their personal relationships. No other approach was taken by more than one-third of people who used this strategy. About 20% of those worldwide who have experienced anxiety or depression fall into this cluster, but it was most common in the Middle East/North Africa (36%), East Asia (28%) and Sub-Saharan Africa (27%).
Table 3.2: Primary clusters of approaches to alleviating anxiety or depression, global results
Percentage of people within each cluster who answered ‘yes’.
When you were feeling so anxious or depressed, did you ever do any of the following to make yourself feel better?
| Cluster 1 holistic combination |
Cluster 2 lifestyle changes |
Cluster 3 primary support from friends or family |
|
|---|---|---|---|
| Talked to a mental health professional | 100% | 0% | 0% |
| Engaged in religious/spiritual activities | 58% | 39% | 25% |
| Talked to friends or family | 89% | 81% | 60% |
| Took prescribed medication | 81% | 32% | 0% |
| Improved healthy lifestyle behaviours | 94% | 100% | 28% |
| Made a change to work situation | 71% | 57% | 32% |
| Made a change to personal relationships | 81% | 67% | 41% |
| Spent time in nature/the outdoors | 91% | 100% | 32% |
Further analysis sheds light on how other factors influenced people’s approaches to feeling better
The above analysis makes it clear that the actions people took to alleviate anxiety or depression were not randomly distributed or independent from each other. Additional analyses were conducted to further explore how other factors impacted the use of each of the eight approaches listed in the survey. The factors with the strongest effects were as follows:
Region
There were wide regional disparities related to country income level for some approaches (as shown in Table 3.1), including:
- Talking to a mental health professional was most likely in Northern America and Europe and least likely in Sub-Saharan Africa.
- Engaging in religious/spiritual activities was most likely in Sub-Saharan Africa and the Middle East/North Africa and least likely in Europe.
Gender
Most approaches had weaker gender-related effects, with two exceptions:
- Men were much more likely than women to report that they had made a change to their work situation, largely reflecting higher rates of formal employment among men in most regions.
- Women were more likely than men to have talked to a mental health professional.
Age at which people first experienced anxiety or depression
- Those who first experienced these conditions at younger ages were more likely to say they had talked to a mental health professional.
- Those who were older when they first experienced these conditions were more likely to say they had talked to friends or family.
Location
- People living in small towns or rural areas were less likely than those living in urban areas or city suburbs to say they had improved healthy lifestyle behaviours.
Education
- People with higher education levels were more likely to say they had talked to a mental health professional.
- People with lower education levels were more likely to say they had taken prescribed medication.
Within-country income
- People in the top 40% (top two quintiles) of their country’s income distribution were more likely than those with lower incomes to say they had talked to a mental health professional.
Use of other forms of help
The following approaches were most commonly associated with one another:
- talking to a mental health professional and taking prescribed medication.
- improving healthy lifestyle behaviours and talking to friends or family.
- making a change to a work situation and making a change to personal relationships.
- spending time in nature/the outdoors and improving healthy lifestyle behaviours.
The findings in this section are based on a series of multivariate regression models in which people’s likelihood to have taken each approach acts as the dependent variable. See Appendix A for a complete discussion of the analysis and outcomes.
Read all chapters
Endnotes
- OECD-FAO. (2016). OECD-FAO Agricultural Outlook 2016-2025. http://www.fao.org/3/bo092e/bo092e.pdf, p. 60
- Fahmy, D. (2018, July 31). Americans are far more religious than adults in other wealthy nations. Pew Research Center. https://www.pewresearch.org/fact-tank/2018/07/31/americans-are-far-more-religious-than-adults-in-other-wealthy-nations/
- Chaabane, S., Chaabna, K., Abraham, A., Mamtani, R., & Cheema, S. (2020). Physical activity and sedentary behaviour in the Middle East and North Africa: An overview of systematic reviews and meta-analysis. Scientific Reports, 10(1), 9363. https://www.nature.com/articles/s41598-020-66163-x
- Sharara, E., Akik, C., Ghattas, H., & Makhlouf Obermeyer, C. (2018). Physical inactivity, gender and culture in Arab countries: A systematic assessment of the literature. BMC Public Health, 18(1), 639. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5960209/
- Sagar-Ouriaghli, I., Godfrey, E., Bridge, L., Meade, L., & Brown, J. S. L. (2019). Improving mental health service utilization among men: A systematic review and synthesis of behavior change techniques within interventions targeting help-seeking. American Journal of Men’s Health, 13(3), 155798831985700. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6560805/#bibr105-1557988319857009
- Vogel, D. L., Heimerdinger-Edwards, S. R., Hammer, J. H., & Hubbard, A. (2011). “Boys don’t cry”: Examination of the links between endorsement of masculine norms, self-stigma, and help-seeking attitudes for men from diverse backgrounds. Journal of Counseling Psychology, 58(3), 368-382. https://doi.apa.org/doiLanding?doi=10.1037%2Fa0023688
- Sagar-Ouriaghli, I., Godfrey, E., Bridge, L., Meade, L., & Brown, J. S. L. (2019). Improving mental health service utilization among men: A systematic review and synthesis of behavior change techniques within interventions targeting help-seeking. American Journal of Men’s Health, 13(3), 155798831985700. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6560805/